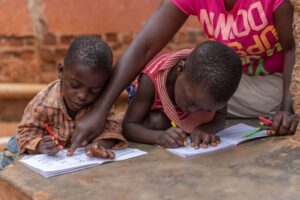
Survey exposes extent of danger to children in Kenya and Uganda
ANALYSIS | MERCY SHIBEMBA | A recent survey which assessed the availability of paediatric antiretroviral formulations across health facilities in Uganda and Kenya has revealed that recommended medications for children were only available in 52% and 64% of Kenyan and Ugandan health facilities.
In the previous year, there had been stock outs of preferred children’s formulations in 40% of Kenyan facilities and 75% of Ugandan facilities.
A stock-out is the absence of required medicines in a health facility, for at least a day. Stock-outs cause delays in starting treatment, incomplete or interrupted treatments, disengagement in care and expenses for patients, which all increase the risk of developing drug-resistance and treatments failing.
Compared to adult medications, child formulations have additional complexities, such as different doses for children of different ages and weights, and many of them having an unpleasant taste.
Their availability is likely to be impacted by the need for cold-storage, shorter shelf-lives, and lower demand. The researchers state that some of the factors driving stock-outs are inefficiencies in supply, dependence on international aid, poor co-ordination with port authorities, a lack of government funding, a lack of forecasting of future needs and a market recovering from the impact of COVID.
There are around 83,000 children (aged 0-14) living with HIV in Kenya and 88,000 in Uganda, out 1.7 million globally. Children living with HIV have increased mortality rates at 5.8%, in comparison to adults at 1.6%. They are also less like to be on treatment than adults (52% vs 76%). Although coverage of paediatric treatment has increased in eastern and southern Africa, from 18% in 2010 to 57% in 2020, 8% of children in the region who are aware of their HIV status are still not on treatment and 15% of those who are on treatment are not virally suppressed.
The researchers’ survey sought to measure availability and stock-outs of paediatric formulations. Independent data collectors visited 144 health facilities, with an even split between Uganda and Kenya. Of these, 110 were public facilities and 34 were private facilities. The sites covered a range of rural and urban communities and reflected both high and low prevalence settings.
The survey asked about medicines which are recommended by the World Health Organization (WHO) as preferred or alternative first- and second-line regimens for infants and children. The team also included questions about formulations suitable for postnatal prophylaxis to prevent vertical transmission of HIV. They also asked about formulations which are only used in limited situations and others which should be phased out.
On the day of the researchers’ visit, the preferred paediatric formulations were available in 52% of facilities in Kenya and 64% of facilities in Uganda. These preferred formulations include abacavir / lamivudine dispersible tablets, dolutegravir dispersible tablets, lopinavir / ritonavir tablets and granules, and zidovudine / lamivudine dispersible tablets, which all children should have access to as first-line or second-line options. The preferred formulations also include oral solutions for nevirapine and zidovudine, each used for postnatal prophylaxis and neonatal treatment.
For example, in Kenya, dolutegravir was available in 70% of facilities and abacavir / lamivudine was available in 90%. However, availability was lower in private facilities in Kenya, at 38% and 63%, respectively. In Uganda, dolutegravir was available in 75% of facilities and abacavir / lamivudine was available in 98%.
The team also surveyed limited-use formulations, which are important for children with extensive resistance or to manage drug-drug interactions. They include darunavir tablets, lamivudine oral solution, nevirapine tablets, raltegravir granules and ritonavir tablets. Average availability was extremely low at
On the other hand, formulations which should be phased out (efavirenz, lopinavir / ritonavir oral solution and ritonavir oral solution) were available in 31% of Kenyan facilities and 11% of Ugandan facilities.
In the previous year, there had been at least one stock-out of preferred use paediatric formulations in 40% of Kenyan facilities and 75% of Ugandan facilities. There were stock-outs of nevirapine oral solution in 43% of Ugandan facilities, but no alternative postnatal prophylaxis formulations were available in more than 5% of sites. There were also stock-outs of dolutegravir / abacavir / lamivudine, which is the WHO-preferred regimen for children aged over 4 weeks of age and weighing less than 30kg. Dolutegravir dispersible tablets had been unavailable in 8% of Kenyan facilities and 32% of Ugandan facilities, while there had been stock outs of abacavir / lamivudine dispersible tablets in 8% and 20% of facilities respectively. Each stock-out lasted for an average of 60 days in Kenya and 37 days in Uganda.
Ultimately, coverage of dolutegravir fell short of meeting the WHO benchmark of 80% availability in both countries. It is of particular concern that there were high rates of stockouts of lopinavir / ritonavir and nevirapine, which are used for postnatal HIV prophylaxis through the breastfeeding period, required by a large number of infants. Potential treatment delays and/or interruptions for newborns can contribute to increased mortality rates, disease progression and HIV transmission.
Whilst the results show reasonable availability of recommended first-line treatments for children in Uganda, this was only the case in public facilities in Kenya, with lower availability in privately-run facilities. Options for second- and third-line treatment in both countries were low, with outdated paediatric formulations still stocked.
Author:: Bagombeka Job